

Alcoholic liver diseases have increased significantly in the last year.
Our report on alcohol use and harm during the COVID-19 pandemic shows an unprecedented increase in deaths from alcohol-related liver disease. In 2020 England registered 5,608 alcohol-related liver deaths, an increase of almost 21% compared to 2019. This is well above the trends before the COVID-19 illness – between 2018 and 2019 the increase was less than 3%.
The 2020 increase in alcohol-related liver deaths came after a 43% increase in alcohol-related liver deaths between 2001 and 2019. This is in stark contrast to other major diseases like heart disease and cancer, where deaths have either remained stable or have decreased.
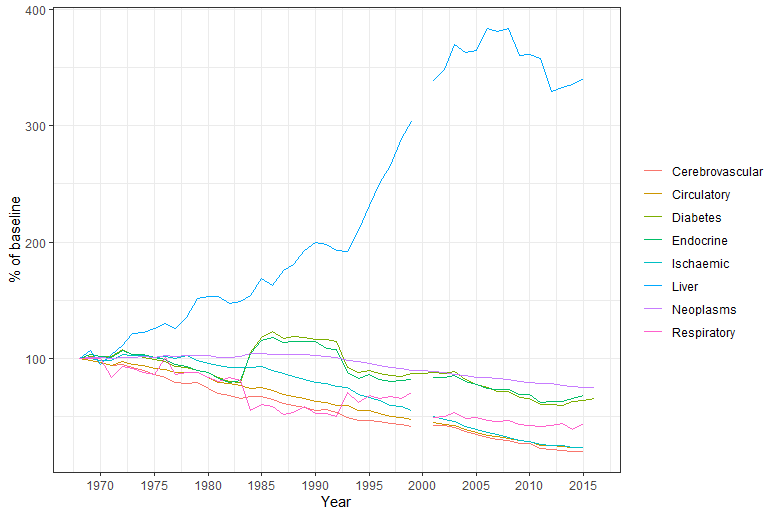
The above data comes from https://gateway.euro.who.int/en/datasets/european-health-for-all-database/. and mecontains the last year with complete data for all indicators (2015). There is no data for the year 2000
Even before the pandemic, liver disease was that second leading cause of premature mortality and years of life lost in England and Wales after ischemic heart disease. And it is will be the main cause within 2 to 3 years. Liver diseases are also now the greatest killer of 35 to 49 year olds in the UK.
People in disadvantaged groups in England are more likely to develop liver disease, be hospitalized and die from it than the wealthiest. In 2020, over half of all alcohol-related liver diseases (57.7%) and deaths (56.5%) occurred in the most deprived 40% of the population.
Why are alcohol-related liver deaths on the rise?
PHEs report observes changes in alcohol consumption during the pandemic and sheds light on the possible reasons for the sharp increase in alcohol-related liver mortality. Based on analysis of off-trade sales data and surveys, there has been an increase in alcohol purchases, consumption and consumption (35+ units per week for women and 50+ units per week for men) since the beginning of the pandemic. This surge was driven by those who were already drinking heavily before the pandemic.
Although alcohol-related cirrhosis can take over a decade to develop, there are people whose livers are already badly damaged can die if they suddenly increase their consumption. Because of this, liver mortality is a quick indicator of changes in alcohol consumption in heavier drinkers.
How can we improve liver supply?
Liver disease is a silent killer. It is mainly caused by alcohol consumption and obesity, and most people with the condition do not know they have it until the disease is at an advanced stage. Research shows that people with advanced liver disease who are hospitalized in an emergency, 7 to 8 times more likely to die than those admitted for stroke or heart attack.
But the liver is an incredible organ. If you stop drinking alcohol or reduce your intake to a low risk level, liver damage can be stopped or even reversed. Once people stop drinking, theirs will long-term survival improves dramatically. But to a third of deaths occur before patients know risk and have the opportunity to stop drinking.
If more professionals routinely ask about alcohol consumption and refer people at higher risk for a liver exam, many premature deaths could be avoided.
A diagnosis of alcoholic liver disease can motivate people to change their behavior. One study reported that around 40% of cirrhotic patients stopped drinking after an initial liver intake. In a community pilot 65% of harmful and addicted drinkers reduced their alcohol consumption after learning, they developed liver fibrosis.
Early diagnosis
An early diagnosis of liver disease offers the possibility of intervention. It gives people access to appropriate medical services that are effective for liver disease. Addicted drinkers with liver disease can get assistance from alcohol treatment services to help them stop drinking.
NICE clinical guidelines on cirrhosis recommends thresholds for referral for liver exam and identifies the specific tests that are able to classify fibrosis and cirrhosis. Standard liver function tests cannot accurately identify early-stage liver damage.
Local public health officers and the NHS should ensure that their liver treatment pathway is the best way to detect fibrosis and cirrhosis in early-stage drinkers at higher risk. You should also ensure that people are receiving adequate support to change their drinking habits and change the course of the disease.
Individual-level interventions such as earlier detection and treatment are important components in reducing alcoholic liver disease.
Population-level interventions are however very effective and cost efficient in lowering alcohol consumption and its associated harm by reducing affordability, reducing availability and limiting marketing exposure. So the most effective response to alcoholic liver disease is a mix of individual to population-based measures.
Would you like to read more about public health? subscribe to our blog here.
Thanks To Source